

In Nairobi’s Mathare estate, 12-year-old Maina wakes each morning with one question quietly weighing on his young mind: how easily will he breathe today?
On good days, he runs to school laughing. On bad days, he slows down, his chest tightening with each shallow breath. His mother has learned to read the signs as a result of the heat, dust, and smoke rising from nearby roads and cooking fires.
“Hot days are the worst, and when it’s dusty, he struggles before he even gets to school,” she says.
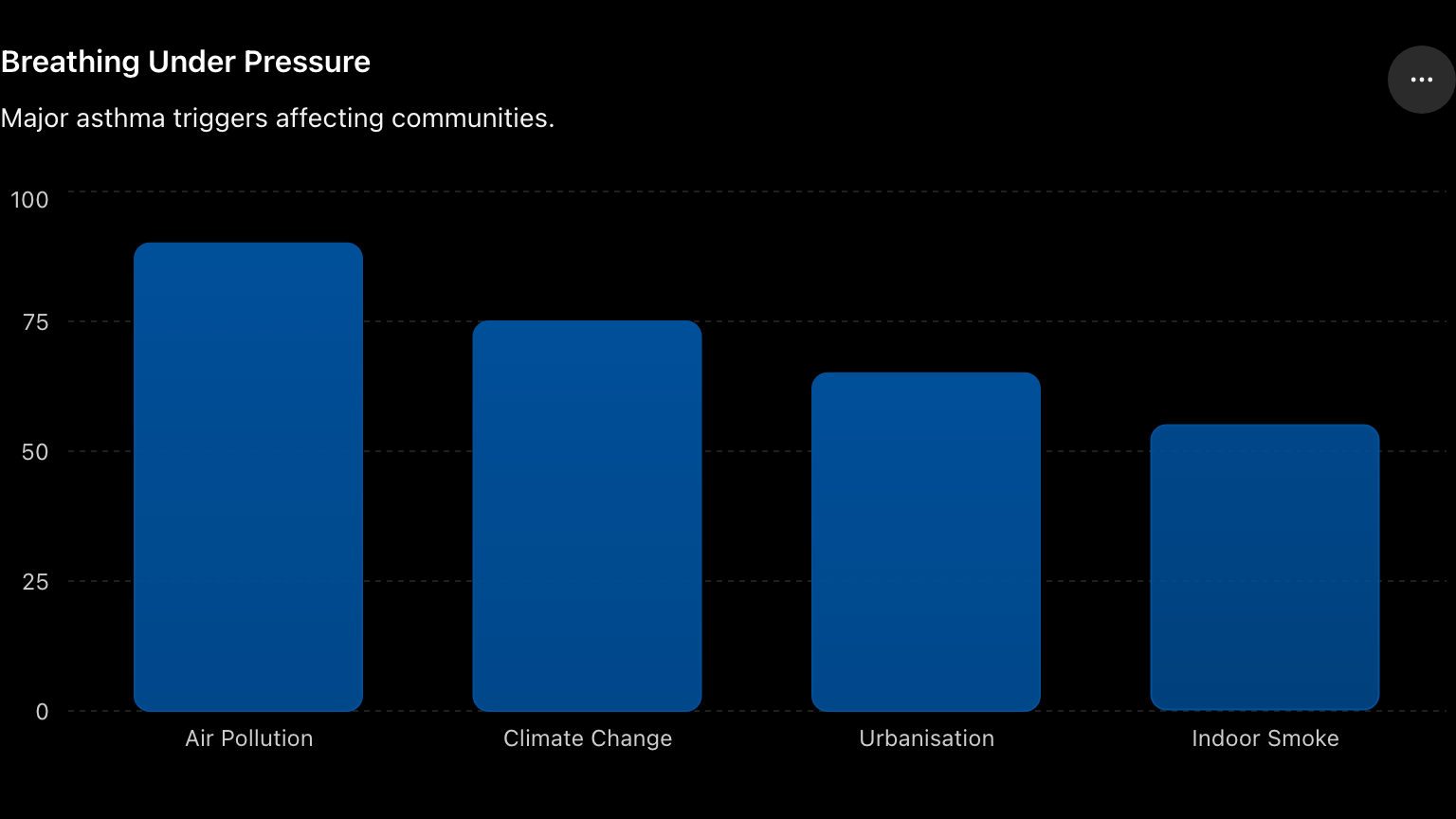
Maina’s experience is becoming common throughout Africa, as asthma and allergy cases continue to rise steadily, with health experts linking the trend to climate change, worsening air pollution, and rapid urbanisation.
According to the World Health Organisation (WHO) Regional Office for Africa, asthma is increasing across the continent, particularly among children, with outdoor pollution, traffic emissions, indoor smoke, and environmental allergens identified as major risk factors.
A study published in The Lancet titled Child and Adolescent Health warns that millions of adolescents in sub-Saharan Africa may be living with undiagnosed asthma. The research, conducted across six countries including Uganda, Ghana, Nigeria, and South Africa, links rising symptoms to rapid urban growth and climate-related environmental changes.
Africa is also warming faster than the global average, intensifying environmental health risks. Scientists increasingly describe asthma as a “climate-sensitive disease,” shaped by shifting temperatures, deteriorating air quality, and changing ecosystems.
Globally, at least 400,000 people die prematurely from asthma each year, according to the WHO, with the greatest burden in low- and middle-income countries.

Air pollution, which is closely tied to climate change, poses an even larger threat. Research published in The Lancet estimates that pollution contributes to around nine million deaths annually worldwide.
In Kenya alone, about 19,000 people die every year due to air pollution exposure, while nine out of ten people breathe air that exceeds WHO safety limits.
The burden is already visible in health systems. According to the Kenya National Bureau of Statistics Economic Survey 2025, respiratory illnesses account for 30.2 per cent of the country’s 66.2 million outpatient visits recorded in 2024. These include asthma, chronic bronchitis, and other pulmonary diseases.
Climate change affects asthma through multiple pathways, and there is evidence to support this.
A study by researchers at the University of Cape Town found that rising temperatures, combined with pollutants such as nitrogen dioxide (NO₂) and fine particulate matter (PM2.5), significantly increase asthma attacks in children. The study, titled “The Interlinkages Between Ambient Temperature and Air Pollution in Exacerbating Childhood Asthma: A Time Series Study in Cape Town, South Africa,” was published on December 1, 2025, in the journal Children.
The researchers analysed more than 7,700 hospital records alongside air quality and weather data, finding that temperature variability, PM2.5, PM10, and NO₂ were all associated with increased childhood asthma exacerbations, especially in urban areas.
Even small environmental shifts matter, with studies showing that slight increases in temperature variability can lead to measurable rises in respiratory hospital admissions.
At the same time, climate change is altering plant biology. Warmer temperatures and rising carbon dioxide levels are increasing pollen production and extending pollen seasons.
According to Professor Mike Levin, a medical specialist and academic in the field of paediatrics and allergy, based at the University of Cape Town, climate change is altering our environment in ways that directly affect respiratory health.
“We are seeing pollen seasons starting earlier, lasting longer, and becoming more intense,” he adds.
In Africa, this effect is magnified. Pollen seasons are already longer than in many regions, making allergies and related asthma often year-round conditions.
“Asthma rarely exists in isolation. It is closely linked to allergies such as pollen, dust mites, mould, and food triggers. There is a very important intersection between food allergy and asthma. The biggest risk factor for dying from a food allergy is having poorly controlled asthma,” says Prof Levin.
This relationship is backed by immunology, as both conditions share overlapping immune pathways. But despite this, diagnosis across the continent remains severely limited.
“There are very few centres across Africa that can properly diagnose and manage food allergies. One in Nairobi, one in Dar es Salaam, two in Lagos, and two in Accra. That’s about it,” Prof Levin says.
A 2022 study titled “Mapping Allergic Diseases in Sub-Saharan Africa,” published in Frontiers in Allergy, confirms this gap. It finds that many African countries lack allergy testing facilities, trained specialists, and confirmatory diagnostic systems.
The study further notes that health systems in Sub-Saharan Africa have historically prioritised infectious diseases such as malaria, tuberculosis, and HIV, leaving allergy care underdeveloped.
Without diagnosis, Prof Levin warns, patients continue to be exposed to triggers unknowingly.
In Kenya, environmental conditions further intensify the problem. Professor Nicholas Oguge, an environmental scientist at the University of Nairobi, identifies transport emissions, industrial activity, and open waste burning as the main drivers of air pollution in Nairobi. He links these directly to asthma, respiratory infections, and cardiovascular disease.
Evidence from air quality studies suggests transport alone contributes roughly 35–40 per cent of PM2.5 pollution in Nairobi, making it the city’s leading source of urban air contamination. These pollutants are well known to inflame airways and trigger asthma attacks.
Dr Andrew Owuor, a Kenyan pulmonologist, observes a direct clinical trend. “The more pollution we have, the more the number of patients presenting with asthma and chronic bronchitis,” he says.
A 2023 Thorax study comparing 2,373 schoolchildren in Nairobi found stark inequalities between informal and affluent areas. Children in informal settlements were exposed to higher pollution levels and reported more asthma-like symptoms, yet were less likely to be formally diagnosed compared to children in wealthier neighbourhoods.

Beyond outdoor pollution, household exposure is also a major driver. Many households in Kenya rely on biomass fuels such as charcoal and firewood, releasing harmful pollutants including carbon monoxide and fine particles. Globally, household air pollution is linked to over 3.8 million deaths annually.
In Kenya, indoor air pollution is especially prevalent in low-income and rural households where ventilation is poor, and exposure is constant.
For children like Maina, exposure does not end outdoors but continues at home. Africa’s rapid urbanisation is expected to intensify these risks. The United Nations projects that Africa’s urban population will rise from 43 per cent in 2020 to nearly 60 per cent by 2050.
According to Prof Levin, urban environments fundamentally reshape immune development.
“Allergies are much more common in urban populations than rural ones, and that’s driven by environmental factors, not genetics.”
He explains that in rural areas, exposure to animals and microbes helps regulate immune responses, while urban environments reduce this exposure and increase pollution-related triggers.
“There’s a strong evolutionary component. The same immune pathways that fight parasites can drive allergic reactions,” he adds.
This may explain why Africa could experience a faster rise in allergic diseases than high-income regions. What makes matters worse is that on the continent, treatment gaps remain.
“Access to inhaled corticosteroids (the ‘brown inhaler ‘) is essential. But access is uneven. Inhalers are often unavailable or unaffordable, and diagnostic tools like spirometers are limited,” says Prof Levin.
A 2019 multi-country study across Sub-Saharan Africa confirms this, finding that inhaled corticosteroids are available in fewer than half of health facilities in some areas, while spirometers are available in less than one-third.
Education is another challenge. “Patients often stop using their medication because they don’t feel immediate effects,” Prof Levin says.
And without consistent treatment, asthma can become life-threatening even when medication is prescribed. Evidence from the WHO shows that asthma can become life-threatening in severe cases and may lead to death if not properly controlled.
Clinical research further indicates that poor adherence to prescribed treatment is a major contributor to severe asthma attacks and preventable fatalities, even among patients who have been diagnosed and given medication.
Looking ahead, experts warn the next decade will be critical. “In the next 10 to 15 years, we are likely to see a significant rise in asthma, eczema, and allergic rhinitis across Africa,” Prof Levin says.
Addressing this crisis will require coordinated action across multiple fronts, moving beyond isolated interventions toward an integrated response.
“This includes reducing transport and industrial emissions through stronger regulation and cleaner technologies, alongside efforts to curb household air pollution,” Prof Levin explains.
At the same time, there is growing emphasis on expanding access to clean cooking fuels, especially in low-income urban settlements where reliance on biomass fuels continues to expose families to harmful indoor air pollution.
Health specialists also stress the need to invest in allergy diagnosis and treatment in systems where respiratory conditions remain widely underdiagnosed.

